My Mum has been suffering with the most horrendous hot flushes and so I bought her a Blue Horizon thyroid test to rule that out as a possible cause.
I am not sure if I made a mistake but she only had water during the 12 hours before bloods were taken (no food) and she had not had her 75mg levothyroxine dose that morning. Can anyone please kindly help with interpreting the attached - she has a GP appointment on the 26th, but is there anything that would warrant more urgent attention please? And also any justification for the hot flushes?!?!
Thank you in advance!
Written by
D0n49
To view profiles and participate in discussions please or .
Hi D0n49Before I was diagnosed I used to get horrendous hot flushes ( not menopausal )especially in bed at night, also my feet used to burn.
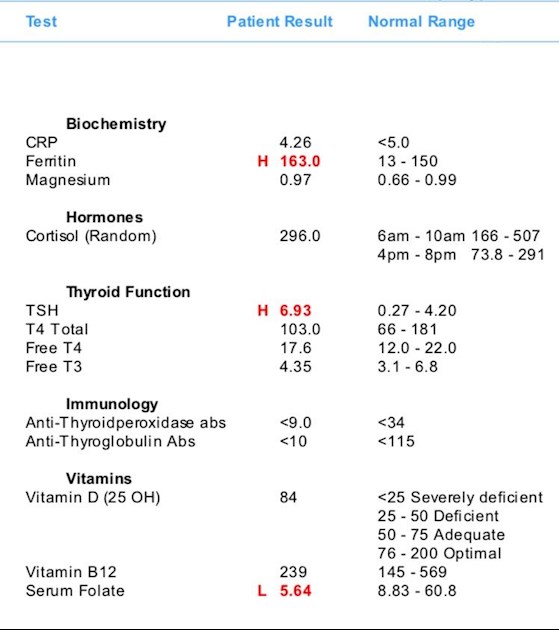
Looking at your mums results I would suggest that she needs an increase in levothyroxine because 75mcg is not really a very big dose and her TSH is way too high for someone who is on thyroid hormones.
How long has she been taking levothyroxine ?
Many people with hypothyroidism need to have their TSH around 1 and at 6.93 I would suggest that your mum's is far too high. There is room for her Free T4 and T3 to go up which may alleviate her symptoms, increases should be in 25 mcg steps and she should have her hormone levels measured 8 weeks after any increase these increases can continue until she is symptom free and her Free T4 and T3 levels are still in range.
The most important thyroid hormone is T3 as this is the one that is active in our body and the lack of it will give us hypothyroid symptoms, the levothyroxine ( T4 ) is inactive and needs to be converted into T3 in our bodies, many people are able to do this especially when we are given enough levo, some people struggle and need supplementary T3.
Your mum's antibody results are negative , but these can fluctuate and some people never have a positive antibody test , this doesn't mean you don't have an autoimmune condition.
Your mum is lucky to have you looking out for her.
Thank you so much knitwitty for your amazing help!
Mum has been on Levothyroxine for as long as I can remember, definitely over 15 years! But as with all her other ailments, I don’t think our GP monitors her as often as they should!
My Mum was hospitalised a couple of weeks ago, they reckon her chest infection moved to her heart which caused it to go into AF! It seems to have settled, thank goodness! And thankfully she did not contract COVID again as they mistakenly placed her on a ward with a positive patient (that was an additional 10 days of hell!)
Could this be the cause of her negative antibody reading perhaps?!?
Her high TSH does not correlate with her FT4 and FT3 levels.
Her CRP is close to the top of the range. As this is an inflammation marker then the lower the better. Her Ferritin is also raised and this can be raised when inflammation or infection is present. Just guessing here but I would say these are connected and I see from the posts in your profile that your mum has COPD and has recently had an exacerbation, also that she had Covid over the Christmas period and was treated for pneumonia. I wouldn't rule out that these illnesses could be disrupting her test results.
Do you know what her TSH, FT4 and FT3 are normally?
Her folate level is below range and should be discussed with her GP. He may or may not decide to prescribe folic acid. If not then she can address this herself.
As for B12, I believe the unit of measurement is pmol/L. If we change that to pg/ml it is 323pg/ml. According to an extract from the book, "Could it be B12?" by Sally M. Pacholok:
"We believe that the 'normal' serum B12 threshold needs to be raised from 200 pg/ml to at least 450 pg/ml because deficiencies begin to appear in the cerebrospinal fluid below 550".
"For brain and nervous system health and prevention of disease in older adults, serum B12 levels should be maintained near or above 1000 pg/ml."
Assuming that she doesn't have any signs of B12 deficiency (if she does, discuss with GP) - you can check that here:
then she could take a sublingual B12 (methylcobalamin) to bring her level up to 550pg/ml and alongside this take a good quality, bioavailable B Complex to balance all the B vitamins. The B Complex will help raise her folate level. After one bottle of B12 this could then be left off and just continue with the B Complex which should further improve her B12 and folate.
When taking B Complex this should be left off for 3-7 days before any blood test as it contains biotin and this can give false results when biotin is used in the testing procedure (which most labs do).
Her Vit D isn't bad but the Vit D Society and Grassroots Health recommend a level of 100-150nmol/L, with a recent blog post on Grassroots Health mentioning a study which recommends over 125nmol/L.
Good levels of Vit D may help boost the immune system. I have COPD and Bronchiectasis and make a point of ensuring my Vit D level remains at the top of the recommended level.I can help with suggestions for improving Vit D if you wish and if she takes D3 she should also take it's important cofactors - magnesium and Vit K2-MK7.
I am not medically trained and my response is based on my own experience and reading.
SeasideSusie, thank you for such a thorough response! Beyond impressed you took the time to read this post let alone the others too - thank you!!!!
Unfortunately I do not know what her levels are normally. It’s only the all too frequent flushes that prompted me to get these tests done for the first time - until now I had foolishly relied on my GP, but they continue to fail my Mum with their lack of care 🥺
Will check out the links to see if she is displaying signs of B12 deficiency- thank you.
Her vitamin D is only what it is as she is currently on Calci-D chewable tablets, otherwise I think it was pretty low after the COVID! I had started both of my parents on 1000IU vitamin D at the very beginning of lockdown, but they did not agree with my Mum so she stopped. My Dad was also on inhalers for his COPD in addition to the vitamin D - so although he was COVID positive over Christmas too he was not as ill as us!
I am not sure whether my Mum has COPD and was undiagnosed, or if COVID triggered it, but it breaks my heart now she is always breathless and wheezy (and I blame myself she contracted COVID 😢)
I am very conscious her immune system is extremely low, her recent bout of illness started with just a sore throat, so any advice would be very gratefully received!
Can’t thank you enough! I feel like a nuisance when I post on here, but I feel abandoned by our GP - so thank you for your time and advice!!!
Her vitamin D is only what it is as she is currently on Calci-D chewable tablets, otherwise I think it was pretty low after the COVID!
Is that prescribed?
Does she take this 4 hours away from her Levo?
Was her calcium tested? It should be before taking calcium.
Was her Vit D tested?
That contains 1000mg calcium and either 800iu or 1000iu Vit D.
I had started both of my parents on 1000IU vitamin D at the very beginning of lockdown, but they did not agree with my Mum so she stopped.
What was this supplement - tablets, capsules, softgels, oral spray? Softgels are the purest and generally contain no excipients that may cause problems.
If she wants to improve her Vit D level to the recommended level then 2,000iu would be a more realistic dose to increase her level. 800-1000iu is just a maintenance dose (and some of us need a higher maintenance dose than that).
Doctors don't know, because they're not taught much about nutrients, but there are important cofactors needed when taking D3. You will have to buy these yourself.
D3 aids absorption of calcium from food and Vit K2-MK7 directs the calcium to bones and teeth where it is needed and away from arteries and soft tissues where it can be deposited and cause problems such as hardening of the arteries, kidney stones, etc.
D3 and K2 are fat soluble so should be taken with the fattiest meal of the day, D3 four hours away from thyroid meds if taking D3 as tablets/capsules/softgels, no necessity if using an oral spray.
For D3 I like Doctor's Best D3 softgels, they are an oil based very small softgel which contains just two ingredients - D3 and extra virgin olive oil, a good quality, nice clean supplement which is budget friendly. Some people like BetterYou oral spray but this contains a lot of excipients and works out more expensive.
For Vit K2-MK7 I like Vitabay or Vegavero brands which contain the correct form of K2-MK7 - the "All Trans" form rather than the "Cis" form. The All Trans form is the bioactive form, a bit like methylfolate is the bioactive form of folic acid.
Magnesium helps D3 to work. We need magnesium so that the body utilises D3, it's required to convert Vit D into it's active form, and large doses of D3 can induce depletion of magnesium. So it's important we ensure we take magnesium when supplementing with D3.
Magnesium comes in different forms, check to see which would suit best and as it's calming it's best taken in the evening, four hours away from thyroid meds if taking magnesium as tablets/capsules, no necessity if using topical forms of magnesium.
It may be worth asking GP to do an iron panel, this will test serum iron, transferrin saturation percentage, total iron binding capacity and ferritin. As it may be possible her ferritin is raised due to infection or inflammation, her normal level may be low enough to cause breathlessness. It's worth ruling this out.
Also, breathlessness can be linked to heart, so maybe ask GP to also check that. Does she have any swelling in ankles, feet or legs? That can be a clue.
As I said before, I'm not diagnosing but these are all things linked and investigated with my own problems.
Here are some things I do to ensure my immune system is as strong as possible:
Vit C - I take 1,000-2,000mg daily
Vit D - I supplement with D3 softgels and keep as close to 150nmol/L as I can, testing twice a year to check level
Allicin (Garlic) liquid - said to be more effective than garlic capsules/softgels, I take one teaspoonful of Allicin liquid daily (I use Allimed from allicin.co.uk). One teaspoonful in a small glass of orange juice and you don't notice it, no aftertaste or garlic breath. Not cheap but I wouldn't be without it.
Oil of Oregano capsules - if I feel any kind of cold, chest or lung infection coming on I start taking these.
SeasideSusie, this is an amazing response, thank you so very much for sharing your wisdom 🙏🏻
After being discharged from having COVID at the start of the year, her blood tests revealed her vitamin D was low. I asked the GP if there was a more agreeable form of supplement she could take as the Vitabiotics 1000IU tablets brought her out in a terrible rash. So they gave her the chewable tablets.
She takes lansoprazole at about 6/6.30am, and then waits half an hour before and she takes the levothyroxine with food. At the same time she takes bisoprolol and ramipril. She used to take the Cacli-D tablets mid morning after she has had her Prednisolone and fluticasone furoate/vilanterol inhaler (not sure how well that works?!) and brushed her teeth. But after the hospital gave her all her tablets together at the same time, more recently she has been doing that!
Will check out the vitamin D gels, K2-MJ7 and magnesium thank you!!!
She had a triple heart bypass 4+ years ago, and the recent chest infection went to her heart and caused it to go back into AF for a while, which is why she was admitted to hospital just over two weeks ago - so yes, she does have heart issues. But they increased her bisoprolol, and except for a couple of occasions her heart seems to be behaving again.
She doesn’t have swollen ankles generally, but she has the the most awful swollen knee - she needs a replacement. Her botched up hip replacements (three times) left her left leg significantly shorter, and it has caused wearing of her right knee where it offsets! But with her medical history, she/they are reluctant to operate, so she is in chronic pain EVERY day with a hip replacement that is working loose, worn knee and arthritic wearing of the spine 🥺 This is why I have been desperate to see if her thyroid was causing the crazy hot flushes, on top of everything else she has to put up with!
We had just assumed the breathlessness was due to the lung damage caused by COVID/her COPD. If this is not the case it would be amazing to get this resolved, thank you! She was meant to have a GP appointment two weeks after her hospital discharge, but that was last Thursday. Chased and she now has an in person one for the end of the month - I have already forwarded the blue Horizon results so will be sure the raise the points you made, if they let me in (they still operate a one in one out policy).
Thank you for everything you have advised!!! I am touched there is someone as helpful as you to take the time to give this brilliant advice!!!
That's quite a cocktail there and we have to be careful with timing of Levo and other medication.
Levo should be taken on it's own, on an empty stomach, one hour before or two hours after food. It should be taken with water only and then water only one hour each side. This is so that nothing affects it's absorption.
Levo should be taken 2 hoursaway from most supplements and other medication but some need 4 hours. Again, this is so that nothing affects it's absorption.
Those needing 4 hour gap from Levo are (they wont all apply to your mom):
Calcium
Vit D
Magnesium
Iron
Oestrogen
HRT
PPIs (Omeprazole, Lansoprazole, etc)
The fluticasone furoate/vilanterol (I expect this is Ellipta) is a steroid inhaler. Have you checked the patient information leaflet and the cautions? I would do so, there should be a section on cardiovascular effects. Also look at interactions with other medications as it mentions betablockers.
Is her potassium level monitored? It should be whilst on this.
Not everyone needs a steroid inhaler, has she seen a lung consultant? Mine said I am not a candidate for steroid inhalers and I'm very glad about that!
Is the Prednisolone a permanent or temporary medication?
Prednisolone can reduce TSH level and if her GP only looks at TSH to determine dose then this may mean a reduction in her Levo which might not be warranted, this is where making sure the FT4 and FT3 are taken into account.
She takes lansoprazole at about 6/6.30am, and then waits half an hour before and she takes the levothyroxine with food. At the same time she takes bisoprolol and ramipril.
The Lansoprazole needs to be taken 4 hours away from Levo.
Levo should be taken one hour before or two hours after food and no other medication or supplements taken with it.
Bisoprolol and ramipril should be taken 2 hours away from Levo.
She used to take the Cacli-D tablets mid morning
Does she need the calcium? Has this been tested and is it being monitored? We should not take calcium unless it is tested and found to be needed. Unless calcium is directed to the right place (bones and teeth) it can be deposited in the wrong places like arteries and soft tissues and cause problems like calcification of arteries, kidney stones, etc. Vit K2-MK7 does this job but doctors don't know about this because they aren't taught much, if anything, about nutrition.
Is she on painkillers? If so check them out for any interaction or problems with absorption of any of her other medications.
It might be worth trying to set up a timetable for your mom's medication.
Does she regularly need a visit to the bathroom during the night? If so she could take her Levo then and this keeps it away from all other medication and food/drink. Or she could take it at bedtime as long as no medication is taken at the same time, and no coffee, tea, hot chocolate, just water.
This is how I take mine, and I take I take 2 x inhalers (non-steroid) and Bisoprolol:
5am-ish (bathroom trip) - Levo
On waking (7am-8am-ish) - Bisoprolol
Washing/showering (1/2 to 1 hour after waking) - inhaler
Breakfast - some supplements including B vitamins and Vit D
Evening meal - Vit K2-MK7
8pm-ish - inhaler
Before bed - magnesium
Vit C I use powder and make up a drink with water and sip throughout the day.
I am not medically qualified so please look into all these things and satisfy yourself that it is suitable for your mom's situation. I have based my response on what I have learned through necessity regarding my own medical conditions.
A pharmacist should be able to advise about the different medications, whether they will interact in any way and whether they should be taken at different times. They tend to know more about these things than doctors. And hospitals tend to give everything at the same time because they only do medication rounds at set times, regardless of whether they interact or cause problems.
Thank you once again! We were not aware of the timing issues, but I have always been concerned about interactions with other medications. So as a suggested I will try and see if the Pharmacist could help!
Thank you for the guidance on what and when you take your medication/supplements. In addition to those medications already mentioned she also takes rivaroxaban (blood thinners), atorvastatin, tramadol and very occasionally MST. The steroids and antibiotics are from her emergency pack, which have been used more often that I would like lately 🥺
I am not sure about her calcium, but her potassium was actually on the high side when she was in hospital three weeks ago - I do not believe the GP is closely monitoring anything!
She was prescribed a steroid inhaler by the Respiratory Consultant, who signed her over to our GP in January after being discharged from the COVID ward. Coincidentally I had a call from the surgery yesterday, and my Parents have a COPD review Wednesday so I am hoping they get the nice Nurse 🤞🏻
Looks like I have some investimagating to do! Thank you so very much for everything- it’s great to not feel so alone xx
If you have an underactive thyroid (hypothyroidism), treatment may be delayed until this problem is treated. This is because having an underactive thyroid can lead to an increased cholesterol level, and treating hypothyroidism may cause your cholesterol level to decrease, without the need for statins. Statins are also more likely to cause muscle damage in people with an underactive thyroid.
Personally I wouldn't take statins if you paid me, there is a lot of scaremongering about cholesterol. I will ask greygoose to comment if she is around.
As for the blood thinners, you will have to satisfy yourself about whether or not Vit K2-MK7 should be taken. There are two forms of Vit K - K1 and K2. K1 is the one they give newborn babies to prevent a now rare bleeding disorder called 'vitamin K deficiency bleeding' (or 'haemorrhagic disease of the newborn'. K2 is the form that directs calcium to bones and teeth and away from soft tissues and arteries. Different articles give conflicting information about whether or not K2 should be used when blood thinners are taken so maybe look into this.
According to those labs, your mother is under-medicated. Her FT3 is on the low-side. That would account for her high cholesterol - assuming she does actually have high cholesterol and not an idiot doctor that just hands out statins 'in case'.
Cholesterol is made in the liver, and it is made for a very good reason: we need it. Cell walls are made of cholesterol, as are sex hormones and the brain is partially made of it. Reduce cholesterol to the rediculous levels the-powers-that-be would have us believe is 'normal' will adversely affect all of those things. Plus, taking statins reduces our energy levels by blocking the production of the enzyme Q10 in the cells, and can cause a whole lot of other problems including hot flushes.
High cholesterol levels are not the life-or-death problem that doctors make them out to be. It does not cause heart attacks or strokes. The reason cholesterol is found in the arteries of heart attacks victims is that it is natures sticking plaster. Inflammation damages arteries and the cholesterol comes along to cover up the wound while it heals. When it's healed, the cholesterol is absorbed by the artery walls - which are made of cholesterol anyway. It is the inflammation that causes the dammage, not the cholesterol. People would probably be better off taking high doses of vit C than statins. Or, better still, optimise their FT3.
The problem is not the liver making excess cholesterol. The problem is that when T3 levels are low, the body cannot process and excrete cholesterol efficiently, and it tends to build up in the blood. Raise the FT3 and the cholesterol should drop. Cholesterol is not going to kill you, but the statins just might!
Thank you so much for the words of wisdom! I honestly don’t know about the underlying reason for the statins prescription, but she has a GP appointment next week so maybe I should email a list of questions ahead 🤣
I think that's a very good idea! There are so many questions one could ask. For a start, does she really need all those medications? That's a terrible ong list! And, if she were optimally medicated for her hypothyroidism, she probably wouldn't need half of them!
Forgot to say, not only are statins not recommended for hypos, they're not recommended for women, either. They do nothing to help women. Her doctor should know that!
You don’t say how old your Mum is? could it be menopause? Might be worth considering her getting her Oestrogen levels checked, if it that’s a possibility?
I still get hot flushes, ten years after the menopause ended. They stop in the summer and are at their worst in the winter.I think it must be related to taking thyroid hormone therapy and not quite hitting the right dose all the time.
I’d say your mother needs a dose increase, her TSH is too high and her free T3 is not in the upper third of the range, it should be 5.5 or above by my calculation.
Right now there is no pattern to the flushes, they happen ALL of the time, day and night! And they are soooo bad, and they cause constantly broken sleep.
The GP prescribed Propantheline bromide but these give her the most awful dry mouth that no amount of fluids can take away, and don’t really do much for the flushes - so she has stopped taking them.
Thank you for your help - do you mind me asking what calculation is involved please, or is this experience based?
Thank you for reaching out! I checked this today and she is currently taking Wockhardt 25mcg and Accord 50mcg please. Is it advised brands be consistent usually?
Content on HealthUnlocked does not replace the relationship between you and doctors or other healthcare professionals nor the advice you receive from them.
Never delay seeking advice or dialling emergency services because of something that you have read on HealthUnlocked.

")